374
Views & Citations10
Likes & Shares
Results: Compared to Hispanic in 2005-2006, it was observed that the Hispanic population in the United States showed an increase in U.S. citizenship, longer periods of residence, higher education, and higher family incomes in 2015-2016, along with a shift towards higher percentages of older adults. Speaking Spanish, non-U.S. citizenship, and lack of health insurance were associated with worse self-rated oral health status in both waves, while being foreign-born, having a higher education, and higher family income were associated with better self-rated oral health. In terms of missing teeth, longer stays in the U.S., higher education, and higher family income were associated with a lower risk of missing teeth, while greater age was associated with a higher risk of missing teeth. Being foreign-born played a more significant protective role in self-rated oral health in the later wave while.
Conclusions: Compared to Hispanics in 2005-2006, respondents in 2015-2016 present higher acculturation and socioeconomic status. The effects of socioeconomic status on oral health outcomes did not change in a decade whereas the roles of foreign-born status and Spanish-speaking were different between waves.
Keywords: Period effects, Oral health, Hispanics, Household language, Non-U.S. citizen, Foreign-born status, Education, Family income
There are a number of studies presented social determinants and health disparities among Hispanics. For instance, Hispanics face numerous challenges in obtaining healthcare and medical services in the United States. Overall, compared to other Americans, the Hispanic population lacks health insurance and preventive medical care [3,4]. Non-citizenship is also one of the major barriers to accessing healthcare, as it disqualifies them from plan eligibility and creates fear of shame and deportation [5]. Language and cultural barriers, as well as high poverty rates and other socio-economic factors, especially among recent Hispanic immigrants, are some of the reasons behind the health disparities between Hispanic Americans and other ethnic groups [3,5].
These health disparities are also reflected in oral health, as literature finds that Hispanic Americans have poorer oral health than White Americans, with more cavities and fewer dental restorations [6]. Compared to non-Hispanic Americans, Hispanic Americans have a lower frequency of dental visits [4]. Compared to non-Hispanic groups, Hispanics are less likely to believe in the need for regular professional dental care, lack knowledge related to oral health, and are unlikely to obtain care [7-9]. The lower frequency of prevention and care results in more oral surgeries for Hispanics [10]. Additionally, even when Hispanics have the same socioeconomic status (SES) as White Americans, SES has weaker protective effects on oral health compared to Whites [11]. Lugo [7] study found that increased care costs and lack of dental insurance were the primary reasons Hispanic Americans did not seek dental care.
As a result of lacking insurance and access to dental care, scholars display that immigrant status was associated with worse oral health among Hispanics. For instance, Hispanics with lower acculturation status report more decayed or missing teeth, as well as higher proportion of periodontics diseases compared to those with high acculturation status. Non-citizen immigrants including Hispanics with no citizenship in the U.S. present significant worse oral health than their native counterparts, whereas such difference disappear when adjusted for health insurance. Previous research also shows evidence on the effects of foreign-born status and language preference on oral health outcomes. For instance, scholars find that Hispanic children from English-speaking households present similar overall health and oral health status as non-Hispanic White children. Scholars have found that children from non-English homes are less likely to receive routine or preventive dental care, make no dentist visits, and present more early childhood caries.
In addition, disparities in oral health are also intergenerationally transmitted. Compared to non-Hispanic Whites, Hispanic children are at the highest risk of poor oral health and difficulty accessing dental care [12,13]. For example, Avila [14] found that language and insurance barriers were the primary factors contributing to the oral health disparities between Hispanic and non-Hispanic children. Additionally, the oral health of Hispanic children is also associated with their parents' cultural adaptation levels; Hispanic children born to parents with high cultural adaptation have better oral health [15].
However, studies have revealed a more complex picture of oral health among Latinx populations when examined from a place of birth perspective. For instance, Sanders [16] uncovered the "Hispanic Paradox" in the field of oral health: despite experiencing poorer socio-economic conditions, higher rates of poverty, and limited access to dental healthcare among foreign-born Hispanic Americans, their oral health outcomes were not only better than those of native-born Hispanics but also outperformed those of non-Hispanic Whites. However, this effect was limited to only first-generation Hispanic individuals. Sanders’ [16] finding from the birthplace perspective suggests a more complex picture of the impact of different structural factors on the oral status of Latinos.
In summary, to examine the oral health status of Hispanics, further examination of the complex relationship between these structural factors and the oral health status of Hispanics in previous studies is needed. In addition, trends in the impact of the above structural factors on oral health disparities among Hispanics need to be considered in the face of demographic, socioeconomic status and the impact of changes in the U.S. health care system over the last 20 years on oral health care (e.g., Affordable Care Act).
This study aims to explore the period effects of oral health disparities among Hispanics in the U.S. and intends to answer three questions about oral health of Hispanics over a decade from 2005 to 2015: first, is there any difference in characteristics among Hispanics from 2005 to 2015 in immigrant status and socioeconomic status (SES)? Second, is there any difference in oral health outcomes among Hispanics from 2005 to 2015? Third, are there differences of the roles of immigrant status and SES in oral health outcomes among Hispanics from 2005 to 2015? [17].
METHODS
Data and Sample: Data were drawn from the National Health and Nutrition Examination Surveys (NHANES). NHANES intends to investigate the health and nutritional status of both adults and children across the United States. Two waves were included wave 2005-2006 and 2015-2016. In each wave, the demographic data, the questionnaire data, and the examination data are included. Only Hispanic adults older than 20 were included in each wave. Among all qualified respondents, those whose information included any missing data in dependent variables or independent variables were excluded. The final interview sample consisted of 1036 respondents in the 2005-2006 wave and 1322 respondents in the 2015-2016 wave.
Measurements
Dependent variables: Self-rated fair/poor oral health. Respondents were asked to “rate the health of your teeth and gums-excellent, very good, good, fair or poor?” Responses were recoded as excellent, very good, good, fair, and poor. In this study, the self-rated oral health was recoded as a binary variable. Responses of excellent, very good, and good are coded as 0, fair and poor are coded as 1. Number of missing teeth. The information about the number of missing teeth was obtained from the examination datasets of NHANES. If a tooth is completely present, it is coded as 1, otherwise, all decayed or lost teeth are coded as 0. Then, the values of all teeth are added up together except the four third molars. The final number of missing teeth is calculated as 28 minus the number of complete teeth.
Independent variables
Respondents who speak Spanish in the interview were coded as no English at home (1), and those who speak English in the interview were coded as English at home (0). Citizenship status is recoded as non-citizens (1) and citizens (0). Country of birth is coded as foreign born (1) and born in the U.S. (0).
- To capture socioeconomic status, this paper measured education and family income. Education is measured in four ordinal categories: no high school (1), high school (2), some college or AA degree (3), and college graduate or above (4). Family income is collapsed into these 4 groups: $0-19,999 (1); $20,000-44,999 (2); $45,000-74,999 (3); $75,000- $ 100,000 and over (4).
- Demographic characteristics included marital status, gender and age. Marital status is coded as married or living with partners (0), and single (1), which includes divorced, widowed, and those who never got married). Gender is coded as female (1) and male (0). Age was recoded as three age groups: 20-39 (1), 40-59 (2), and older than 60 (3).
Statistical Analysis
The data analyses were performed using the STATA software version 14.0. Three stages were employed to process the analysis. First, the authors reported the percentages, as well as mean and standard deviation (only for the number of missing teeth) of Hispanics in each wave. Second, the authors applied logistic regression models for the self-rated oral health for each wave. Third, Poisson regression models were used to estimate the effects of independent variables on the number of missing teeth for each wave. The sample weight was applied. Slope difference between waves was tested by the formula: t= (b1-b2)/√(SE12+SE22). The letter b is the coefficient and SE refer to the standard error of b.
RESULTS
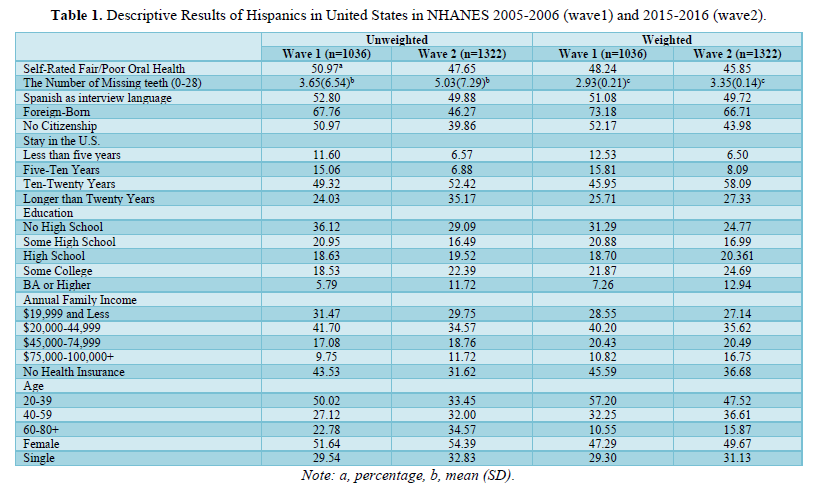
Table 1 presents the descriptive results of the Hispanic population in the United States in NHANES 2005-2006 (wave 1) and 2015-2016 (wave 2), both unweighted and weighted. In terms of self-rated oral health, the percentage of Hispanics who rated their oral health as fair or poor was slightly higher in wave 1 (50.97%) than in wave 2 (47.65%). When the data were weighted, the percentages were 48.24% for wave 1 and 45.85% for wave 2. The mean number of missing teeth for Hispanic adults was 3.65 (SD=6.54) in wave 1 and 5.03 (SD=7.29) in wave 2 in unweighted data. The mean number of missing teeth was 2.93 (SE=0.21) in wave 1 and 3.35 (SE=0.14) in wave 2 in weighted data.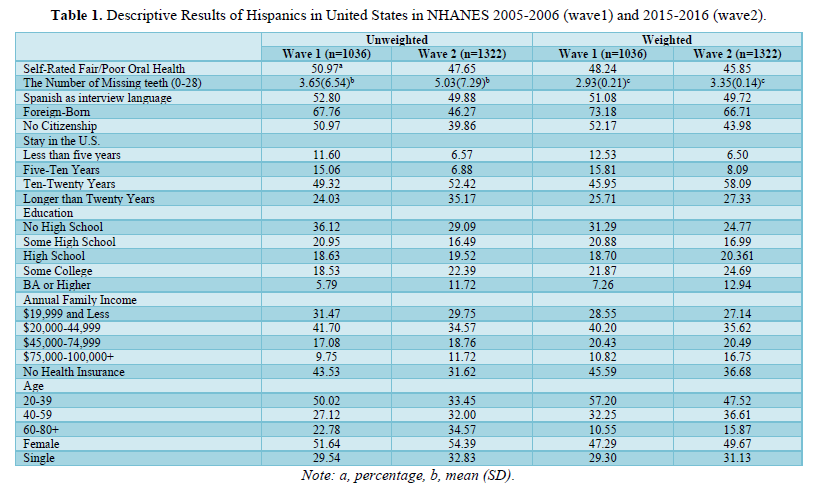
Spanish was the interview language for approximately 50% of participants in both waves. The percentage of Hispanics with U.S. citizenship is higher in wave 2 than in wave 1. In wave 2, more participants had stayed in the U.S. for longer than 20 years. The percentage of participants with no high school education decreased from wave 1 to wave 2, while the percentage with a BA or higher increased. The percentage of participants with an annual family income of $19,999 or less decreased from wave 1 to wave 2, while the percentage with an annual family income of $75,000 or more increased. Compared to wave 1, wave 2 has a lower percentage of Hispanic adults aged 20-39 and a higher percentage of Hispanic adults aged 60 and older.
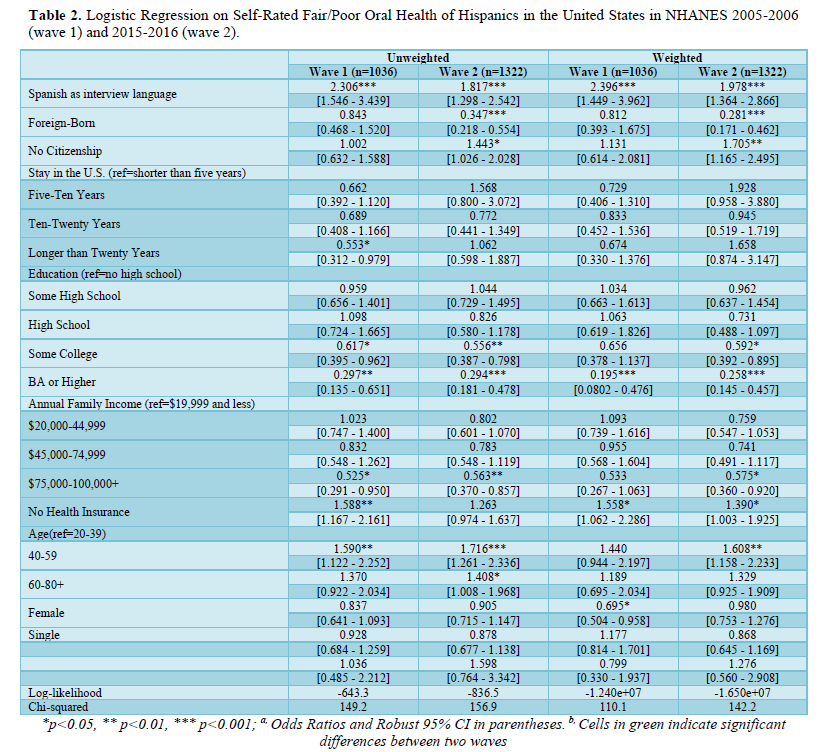
Table 2 presented the logistic regression analysis on the self-rated fair/poor oral health of Hispanics in the United States in NHANES 2005-2006 (wave 1) and 2015-2016 (wave 2). The analysis includes both unweighted and weighted data. Speaking Spanish, non-U.S. citizenship, and lack of health insurance were associated with worse self-rated oral health status in both waves of the study. Being foreign-born was associated with better self-rated oral health in wave 2 only.
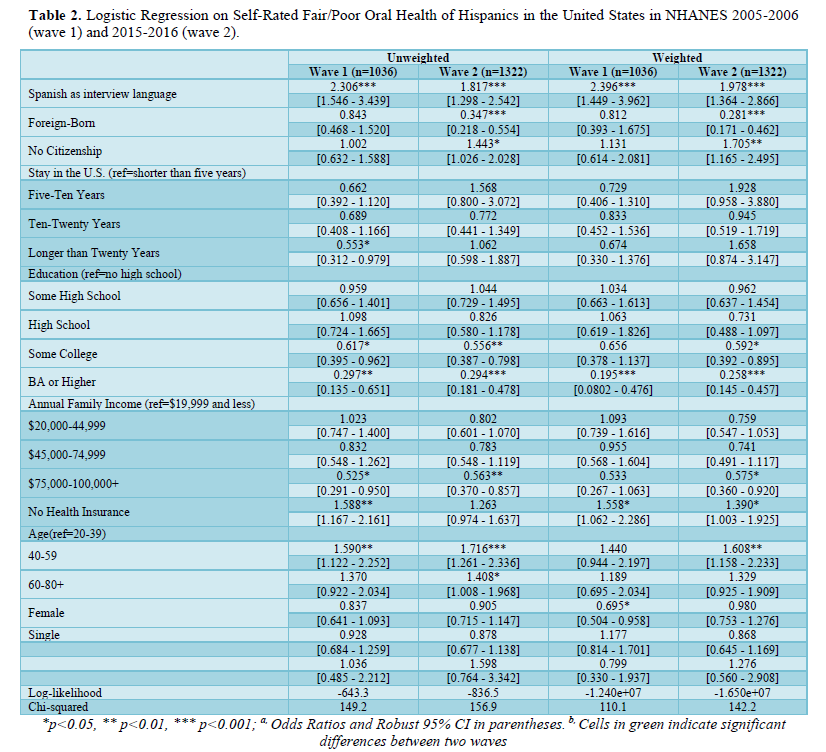
In addition, having a bachelor's degree or higher was associated with better self-rated oral health status in both waves. Family income was also associated with self-rated oral health status, but this relationship varied depending on whether the data was weighted or unweighted. For the unweighted data, higher family income was associated with better self-rated oral health status, while for the weighted data, this relationship was only significant in wave 2. Age was found to be significantly associated with self-rated oral health status, with older respondents (40-59 years old) more likely to report fair/poor oral health compared to younger respondents (20-39 years old). The test of slope between waves suggested that being foreign-born played a more significant protective role in self-rated oral health in the later wave.
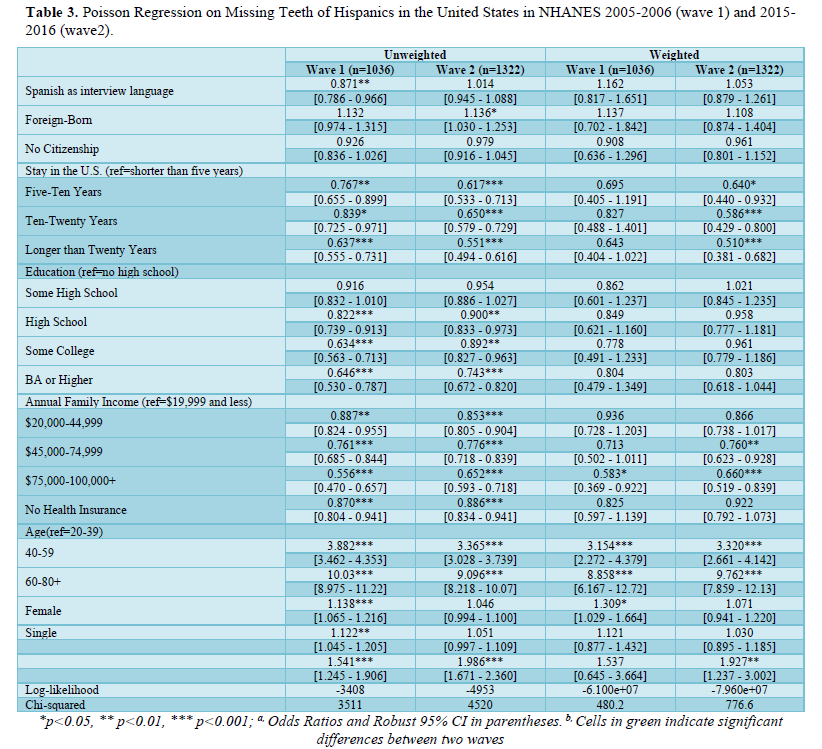
Table 3 presented the results of Poisson regression models conducted on missing teeth of Hispanics in the United States. The data come from wave 1 and wave 2. The table reports unweighted and weighted estimates for various predictors. The results indicate that for unweighted data, longer stays in the U.S. were associated with a lower risk of missing teeth in both waves. However, for weighted data, long stays in the U.S. were only associated with a lower risk of missing teeth in wave 2.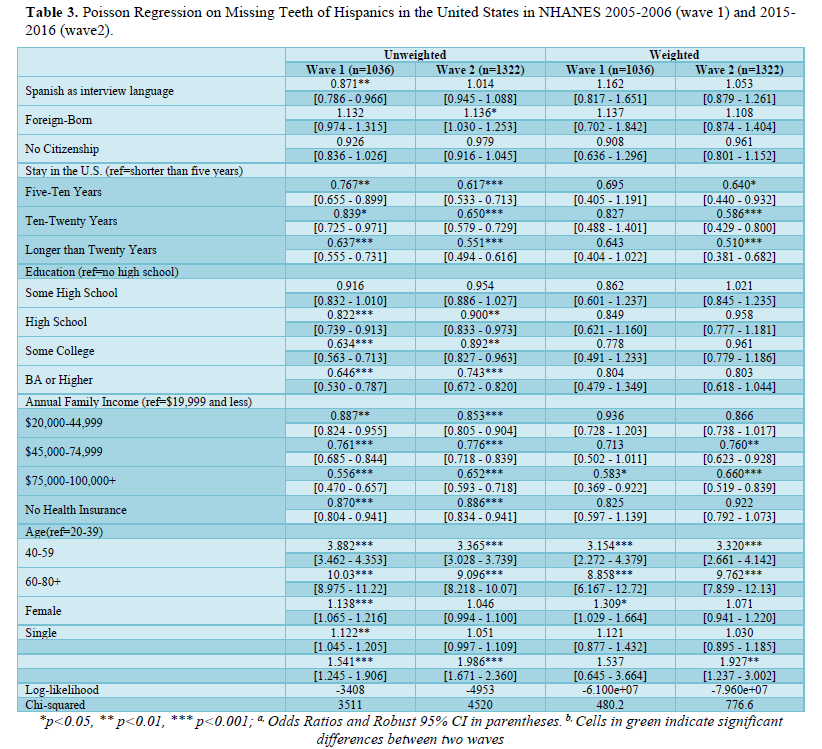
Higher education was found to be associated with a lower risk of missing teeth in both waves for unweighted data, but not for weighted data. Similarly, for unweighted data, higher family income was associated with a lower risk of missing teeth in both waves, whereas for weighted data, only an annual household income of $75,000 and above was associated with a lower risk of missing teeth in both waves. For unweighted data, lack of health insurance was associated with a lower risk of missing teeth in both waves, whereas for weighted data, this association was not significant in either wave. Greater age was found to be associated with a higher risk of oral health problems in both waves. In wave 1, women had a higher risk of missing teeth; however, there was no significant association between being female and the risk of missing teeth in wave 2. For unweighted data, the test of slope between waves suggested that staying in the U.S. in ten-twenty years played a more significant protective role in self-rated oral health in the later wave.
DISCUSSION AND CONCLUSION
In this paper, we presented population change of Hispanics from 2005 to 2015 and tested the different effects of immigrant status and social status on oral health outcomes in a decade. Compared to Hispanics documented in the 2005-2006 wave data, those who were included in 2015-2016 wave present more missing teeth, lower proportion of Spanish speaking, being foreign-born, and lack of U.S. citizenship. On the other hand, the length of stay in the U.S, the education levels, family income, and coverage of health insurance increased compared to a decade ago. Moreover, Spanish-speaking and no insurance were associated with worse self-rated oral health in both waves, whereas staying longer time in the U.S, college education, and high level of family income (higher than $75,000) presented protective effects on fair/poor self-rated oral health. Being foreign-born present significantly greater protective effect in 2015-2016 wave than that in 2005-2006 wave. Length of staying in the U.S, higher levels of education, and family income also present protective effects on missing teeth. The result that no health insurance was associated with more missing teeth was unexpected. One possible explanation is that respondents with no missing teeth were less likely to purchase health insurance.
This study has three limitations. First, dental care was not investigated in wave 2005-2006. To be comparative between waves, we did not include dental care in our model. In addition, several related variables or a number of cases were missing due to non-comparable across waves, such as tooth brushing, smoking, and alcohol consumption. Second, this study focused on the period effects of oral health among Hispanics, whereas it is hard to separate age effects because the proportion of middle and old age respondents in wave 2015-2016 was higher than that in wave 2005-2015. It is hard to exclude the effects of age in the changed pattern of oral health outcomes. Third, the self-rated oral health and other variables are self-reported data, and it is possible that inaccurate information was recorded.
- Nadeem R (2023) A brief statistical portrait of U.S. hispanics. Pew Research Center Science & Society.
- Ruggles S, Flood S, Foster S, Goeken R, Jose Pacas, et al. (2021) IPUMS USA: Version 11.0 [dataset]. Minneapolis, MN: IPUMS.
- Funk C, Lopez MH (2022) Hispanic Americans’ experiences with health care. Pew Research Center.
- Ramos-Gomez F, Cruz GD, Watson MR, Canto MT, Boneta AE (2005) Latino oral health: A research agenda toward eliminating oral health disparities. J Am Dent Assoc 136(9): 1231-1240.
- Pérez‐Escamilla R, Garcia J, Song D (2010) Health care access among Hispanic immigrants: Alguien está escuchando? [Is anybody listening?]. NAPA Bull 34(1): 47-67.
- Wu B, Liang J, Plassman BL, Remle RC, Bai L (2011) Oral health among white, black, and Mexican‐American elders: An examination of edentulism and dental caries. J Public Health Dent 71(4): 308-317.
- Lugo I, Arteaga S, Sanchez V (2014) Oral health status, perceptions, and access to dental care in the Hispanic population. Gen Dent 62(4): 24-30.
- Luciano M, Overman VP, Frasier PY, Platin E (2008) Survey of oral health practices among adults in a North Carolina Hispanic population. Am Dent Hyg Assoc 82(2): 20-20.
- Patino D, McQuistan MR, Qian F, Hernandez M, Weber-Gasparoni K, et al. (2018) Oral health knowledge levels of Hispanics in Iowa. J Am Dent Assoc 149(12): 1038-1048.
- Manski RJ, Moeller JF (2002) Use of dental services: an analysis of visits, procedures and providers, 1996. J Am Dent Assoc 133(2): 167-175.
- Assari S (2018) Socioeconomic status and self-rated oral health; Diminished return among hispanic whites. Dent J 6(2): 11.
- Dye BA (2012) Oral health disparities as determined by selected healthy people 2020 oral health objectives for the United States, 2009-2010 (No. 100). US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics.
- Kopycka-Kedzierawski DT, Billings RJ (2011) Prevalence of dental caries and dental care utilization in preschool urban children enrolled in a comparative-effectiveness study. Eur Arch Paediatr Dent 12(3): 133-138.
- Avila RM, Bramlett MD (2013) Language and immigrant status effects on disparities in Hispanic children’s health status and access to health care. Matern Child Health J 17: 415-423.
- Kabani FA, Stockbridge EL, Varghese BB, Loethen AD (2020) Acculturation and the oral health of a nationally representative sample of Hispanic children in the United States: An analysis of 2011-2012 National Survey of Children’s Health data. BMC Public Health 20(1): 1-12.
- Sanders AE (2010) A Latino advantage in oral health-related quality of life is modified by nativity status. Soc Sci Med 71(1): 205-211.
- Spolsky VW, Marcus M, Der-Martirosian C, Coulter ID, Maida CA (2012) Oral health status and the epidemiologic paradox within Latino immigrant groups. BMC Oral Health 12: 1-7.
-
 Table 1
Table 1 -
Table 2
-
Table 3
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- BioMed Research Journal (ISSN:2578-8892)
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)
- Journal of Allergy Research (ISSN:2642-326X)
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)